What is Crohn's disease?

Crohn's disease (sometimes called Crohn disease) is a chronic inflammatory disease of the intestines. It primarily causes ulcerations (breaks in the mucosal lining) of the small and large intestines but can affect the digestive system anywhere from the mouth to the anus.
Crohn's is also called granulomatous enteritis or colitis, regional enteritis, ileitis, or terminal ileitis.
Related conditions
Crohn's disease is related closely to another chronic inflammatory condition that involves only the colon called ulcerative colitis. Together, Crohn's disease and ulcerative colitis are referred to as inflammatory bowel disease (IBD). Ulcerative colitis and Crohn's disease have no medical cure. Once the diseases begin, they tend to fluctuate between periods of inactivity (remission) and activity (relapse).
What are the differences between Crohn's disease and ulcerative colitis (UC)?
While ulcerative colitis causes inflammation only in the colon (colitis) and/or the rectum (proctitis), Crohn's disease may cause inflammation in the colon, rectum, small intestine (jejunum and ileum), and, occasionally, even the stomach, mouth, and esophagus.
- The patterns of inflammation in Crohn's disease are different from ulcerative colitis. Except in the most severe cases, the inflammation of ulcerative colitis tends to involve the superficial layers of the inner lining of the bowel. The inflammation also tends to be diffuse and uniform (all of the linings in the affected segment of the intestine are inflamed).
- Unlike ulcerative colitis, the inflammation of Crohn's disease is concentrated in some areas more than others and involves layers of the bowel that are deeper than the superficial inner layers. The affected segment(s) of the bowel in Crohn's disease often is studded with deeper ulcers with normal lining between these ulcers.
What are the types of Crohn's disease?
The different subtypes of Crohn's disease and their symptoms are:
- Crohn's colitis is inflammation that is confined to the colon. Abdominal pain and bloody diarrhea are the common symptoms. Anal fistulae and perirectal abscesses also can occur.
- Crohn's enteritis refers to inflammation confined to the small intestine (the second part, called the jejunum, or the third part, called the ileum). Involvement of the ileum alone is referred to as Crohn's ileitis. Abdominal pain and diarrhea are the common symptoms. Obstruction of the small intestine also can occur.
- Crohn's terminal ileitis is inflammation that affects only the very end of the small intestine (terminal ileum), the part of the small intestine closest to the colon. Abdominal pain and diarrhea are the common symptoms. Small intestinal obstruction also can occur.
- Crohn's enterocolitis and ileocolitis are terms to describe inflammation that involves both the small intestine and the colon. Bloody diarrhea and abdominal pain are the common symptoms. Small intestinal obstruction also can occur.
- Crohn's terminal ileitis and ileocolitis are the most common types of Crohn's disease. (Ulcerative colitis frequently involves only the rectum or rectum and sigmoid colon at the distal end of the colon. These are called ulcerative proctitis and procto-sigmoiditis, respectively.)

QUESTION
What is Crohn's disease? See AnswerWhat causes Crohn's disease?
The cause of Crohn's disease is unknown. Some scientists suspect that infection by certain bacteria, such as strains of mycobacterium, may be the cause of Crohn's disease. Crohn's disease is not contagious. Diet may affect the symptoms of Crohn's disease; however, it is unlikely that diet is responsible for causing the disease.
Immune system
- Activation of the immune system in the intestines appears to be important in IBD. In individuals with IBD, the immune system is abnormally and chronically activated in the absence of any known invader. This results in chronic inflammation and ulceration.
Genetics
- The susceptibility to abnormal activation of the immune system is genetically inherited. Thus, first-degree relatives (brothers, sisters, children, and parents) of people with IBD are more likely to develop these diseases. Recently a gene called NOD2 has been identified as being associated with Crohn's disease. This gene is important in determining how the body responds to some bacterial products. Individuals with mutations in this gene are more susceptible to developing Crohn's disease.
- Other genes are still being discovered and studied which are important in understanding the pathogenesis of Crohn's disease including autophagy-related 16-like 1 gene (ATG 16L1) and IRGM, which both contribute to macrophage defects and have been identified with the Genome-Wide Association study.
Bacteria
- There also have been studies that show that in the intestines of individuals with Crohn's disease, there are higher levels of a certain type of bacterium, E. coli, which might play a role in the disease. One postulated mechanism by which this could occur is through a genetically determined defect in the elimination of the E. coli, by intestinal mucosal macrophages. The exact roles that these various factors play in the development of this disease remain unclear.
Who is more likely to develop Crohn's disease?
Risk factors for Crohn's disease include the following:
- Men and women are affected equally by inflammatory bowel disease.
- Americans of Jewish European descent are more likely to develop IBD than the general population. IBD has historically been considered predominately a disease of Caucasians, but there has been an increase in the reported cases in African Americans. The prevalence appears to be lower among Hispanic and Asian populations.
- IBD most commonly begins during adolescence and early adulthood (usually between the ages of 15 and 35). There is a small second peak of newly diagnosed cases after age 50.
- The number of new cases (incidence) and the number of cases (prevalence) of Crohn's disease in the United States are rising, although the reason for this is not completely understood.
- Crohn's disease tends to be more common in relatives of patients with Crohn's disease. If a person has a relative with the disease, his/her risk of developing the disease is estimated to be at least 10 times that of the general population and 30 times greater if the relative with Crohn's disease is a sibling. It also is more common among relatives of patients with ulcerative colitis.
Health News
- More of America's Pets Are Overdosing on Stray Coke, Meth
- GLP-1 Zepbound Is Approved As First Drug For Sleep Apnea
- Feeling Appreciated by Partner is Critical for Caregiver's Mental Health
- Tips for Spending Holiday Time With Family Members Who Live with Dementia
- The Most Therapeutic Kind of Me-Time
 More Health News »
More Health News »
What are the symptoms of Crohn's disease?
The symptoms of Crohn's disease are dependent on the location, the extent, and the severity of the inflammation.
Common symptoms and signs of Crohn's disease include:
- Abdominal pain
- Diarrhea
- Weight loss
Less common signs and symptoms include:
- Poor appetite
- Fever
- Night sweats
- Rectal pain
- Occasionally rectal bleeding
Other symptoms
Up to one-third of patients with Crohn's disease may have one or more of these conditions, symptoms, and signs that involve the anal area affected.
- Swelling of the tissue of the anal sphincter, the muscle at the end of the colon that controls defecation.
- Development of ulcers and fissures (long ulcers) within the anal sphincter. These ulcers and fissures can cause bleeding and pain with defecation.
- Development of anal fistulae (abnormal tunnels) between the anus or rectum and the skin surrounding the anus). Mucous and pus may drain from the openings of the fistulae on the skin.
- Development of perirectal abscesses (collections of pus in the anal and rectal area). Peri-rectal abscesses can cause fever, pain, and tenderness around the anus.
How do you get a Crohn's disease diagnosis? Is there a test?
There is no specific diagnostic test for Crohn’s disease. The diagnosis of Crohn's disease is suspected in patients with fever, abdominal pain and tenderness, diarrhea with or without bleeding, and anal diseases, such as ulcers or fissures.
- Laboratory blood tests may show elevated white blood cell counts and sedimentation rates, both of which suggest infection or inflammation. Other blood tests may show low red blood cell counts (anemia), low blood proteins, and low body minerals, reflecting loss of these minerals due to chronic diarrhea.
- Barium X-ray studies can be used to define the distribution, nature, and severity of the disease. Barium is a chalky material that is visible by X-ray and appears white on X-ray films. When barium is ingested orally (upper GI series) it fills the intestine, and pictures (X-rays) can be taken of the stomach and the small intestines. When barium is administered through the rectum (barium enema), pictures of the colon and the terminal ileum can be obtained. Barium X-rays can show ulcerations, narrowing, and, sometimes, fistulae of the bowel.
- Direct visualization of the rectum and the large intestine can be accomplished with flexible viewing tubes (colonoscopes). A colonoscopy is more accurate than barium X-rays in detecting small ulcers or small areas of inflammation of the colon and terminal ileum. Colonoscopy also allows for small tissue samples (biopsies) to be taken and sent for examination under the microscope to confirm the diagnosis of Crohn's disease. Colonoscopy also is more accurate than barium X-rays in assessing the degree (activity) of inflammation.
- Computerized axial tomography (CAT or CT) scanning is a computerized X-ray technique that allows imaging of the entire abdomen and pelvis. It can be especially helpful in detecting abscesses. CT and MRI enterography are imaging techniques that use oral contrast agents consisting of watery solutions with or without low concentrations of barium to provide more adequate luminal distension, which has been reported to be superior in the evaluation of small bowel pathology in patients with Crohn's disease.
- Video capsule endoscopy (VCE) has also been added to the list of tests for diagnosing Crohn's disease. For video capsule endoscopy, a capsule containing a miniature video camera is swallowed. As the capsule travels through the small intestine, it sends video images of the lining of the small intestine to a receiver carried on a belt at the waist. The images are downloaded and then reviewed on a computer. The value of video capsule endoscopy is that it can identify the early, mild abnormalities of Crohn's disease. Video capsule endoscopy may be particularly useful when there is a strong suspicion of Crohn's disease but the barium X-rays are normal. (Barium X-rays are not as good at identifying early, mild Crohn's disease.) In a prospective blinded evaluation, video capsule endoscopy was demonstrated to be superior in its ability to detect small bowel pathology missed on small bowel radiographic studies and CT exams.
- Video capsule endoscopy should not be performed in patients who have an obstruction of the small intestine. The capsule may become stuck at the site of obstruction and make the obstruction worse. Doctors usually also are reluctant to perform video-capsule endoscopy for the same reason in patients whom they suspect of having small intestinal strictures (narrowed segments of the small intestine that can result from prior surgery, prior radiation, or chronic ulceration, for example, from Crohn's disease). There is also a theoretical concern for electrical interference between the capsule and implanted cardiac pacemakers and defibrillators; however, so far in a small-moderate number of patients with pacemakers or defibrillators who have undergone video capsule endoscopy, there have been no problems.
How does Crohn's disease affect the intestines?
Early stages of Crohn's disease
In the early stages, Crohn's disease causes small, scattered, shallow, crater-like ulcerations (erosions) on the inner surface of the bowel.
- These erosions are called aphthous ulcers.
- With time, the erosions become deeper and larger, ultimately becoming true ulcers (which are deeper than erosions), and causing scarring and stiffness of the bowel.
- As the disease progresses, the bowel becomes increasingly narrowed and ultimately can become obstructed.
- Deep ulcers can cause puncture holes or perforations in the wall of the bowel, and bacteria from within the bowel can spread to infect adjacent organs and the surrounding abdominal cavity.
Obstructions in the intestines
When Crohn's disease narrows the small intestine to the point of obstruction, the flow of the contents through the intestine ceases.
- Sometimes, the obstruction can be caused suddenly by poorly digestible fruit or vegetable matter that plugs the already-narrowed segment of the intestine.
- When the intestine is obstructed, food, fluid, and gas from the stomach and the small intestine cannot pass into the colon. The symptoms of small intestinal obstruction then appear, including severe abdominal cramps, nausea, vomiting, and abdominal distention.
- Obstruction of the small intestine is much more likely since the small intestine is much narrower than the colon.
Ulcers in the colon and small intestine
Deep ulcers can cause puncture holes or perforations in the walls of the small intestine and the colon, and create a tunnel between the intestine and adjacent organs. If the ulcer tunnel reaches an adjacent space inside the abdominal cavity, a collection of infected pus (an abdominal abscess) is formed. Individuals with abdominal abscesses can develop tender abdominal masses, high fevers, and abdominal pain.
- When the ulcer tunnels into an adjacent organ, a channel (fistula) is formed.
- The formation of a fistula between the intestine and the bladder (enteric-vesicular fistula) can cause frequent urinary tract infections and the passage of gas and feces during urination.
- When a fistula develops between the intestine and the skin (enteric-cutaneous fistula), pus and mucous emerge from a small painful opening on the skin of the abdomen.
- The development of a fistula between the colon and the vagina (colonic-vaginal fistula) causes gas and feces to emerge through the vagina.
- The presence of a fistula from the intestines to the anus (anal fistula) leads to a discharge of mucous and pus from the fistula's opening around the anus.
Subscribe to MedicineNet's Daily Health News Newsletter
By clicking Submit, I agree to the MedicineNet's Terms & Conditions & Privacy Policy and understand that I may opt out of MedicineNet's subscriptions at any time.
What is the treatment for Crohn's disease?
Since there is no cure for Crohn's disease, the goals of treatment are to do the following:
- Induce remissions
- Maintain remissions
- Minimize the side effects of treatment
- Improve the quality of life
Treatment of Crohn's disease and ulcerative colitis with medications is similar though not always identical; however, no medication can cure Crohn's disease.
- Patients with Crohn's disease typically will experience flares, or periods of relapse (worsening of inflammation) followed by periods of remission (lessening of inflammation) lasting months to years.
- During relapses, symptoms of abdominal pain, diarrhea, and rectal bleeding worsen.
- During remissions, these symptoms improve. Remissions usually occur because of treatment with medications or surgery, but occasionally they occur spontaneously without any treatment.
- Anti-inflammatory agents such as 5-ASA compounds (mesalamine [Asacol HD, Delzicol], sulfasalazine [Azulfidine]) and corticosteroids (prednisone and budesonide [Entocort EC]), antibiotics (ciprofloxacin [Cipro], metronidazole [Flagyl]), immunomodulators (6-MP [6-mercaptopurine] [Purinethol, Purixan], azathioprine [Imuran], methotrexate [Trexall]), and biosimilars (adalimumab [Humira], adalimumab-adbm [Cyltezo], adalimumab-atto [Amgevita], certolizumab [Cimzia], infliximab [Remicade], infliximab-abda [Renflexis], infliximab-dyyb [Inflectra], natalizumab [Tysabri], ustekinumab [Stelara], vedolizumab [Entyvio]) are medications used to treat Crohn’s disease.
The selection of treatment regimens depends on disease severity, disease location, and disease-associated complications.
Various treatment guidelines recommend that approaches be sequential -- initially to induce clinical remission, and then to maintain remissions. Initial evidence of improvement should be seen within 2 to 4 weeks, and maximal improvement should be seen in 12 to 16 weeks. The classic approach to therapy for Crohn's disease has been a "step-up" approach starting with the least toxic agents for mild disease, and increasingly more aggressive treatment for more severe diseases, or patients who have not responded to less toxic agents.
Treatment has been moving toward a "top-down" approach (early aggressive management) that might decrease exposure to anti-inflammatory agents and increase exposure to agents that enhance mucosal healing, which might prevent future complications.
From 
Is there a surgery used to treat Crohn's disease?
There is no surgical cure for Crohn's disease. Even when all of the diseased parts of the intestines are removed, inflammation frequently recurs in previously healthy intestines months to years after the surgery.
Surgery for Crohn's disease is used primarily for the following:
- Removal of a diseased segment of the small intestine that is causing obstruction.
- Drainage of pus from abdominal and perirectal abscesses.
- Treatment of severe anal fistulae that do not respond to drugs.
- Resection of internal fistulae (such as a fistula between the colon and bladder) that are causing infections.
What happens after surgery
- Usually, after the diseased portions of the intestines are removed surgically, patients can be free of disease and symptoms for some time, often years. When successfully performed, surgery can lead to a marked improvement in a patient's quality of life. In many patients, Crohn's disease eventually returns, affecting previously healthy intestines.
- The recurrent disease usually is located at or near the site of surgery. In fact, half of patients can expect to have a recurrence of symptoms within four years of surgery. Drugs such as Pentasa or 6-MP have been useful in some patients to reduce the chances of relapse of Crohn's disease after surgery.
- There is accumulating evidence in favor of post-operative therapy to delay the recurrence of Crohn's disease. There appears to be some benefit of mesalamine in reducing the risk of post-op recurrence for up to 3 years. A study has shown infliximab to be effective in preventing postoperative recurrence after ileocecal resection, though relapse may occur when therapy is stopped.
- Treatment strategies by severity and location of disease (Based on the Second European Evidence-Based Consensus on the Diagnosis and Management of Crohn's Disease.)
Mild to Moderate Active Disease
- Commonly treated with oral mesalamine 3.2-4 g daily or sulfasalazine for ileocolonic or colonic disease as 3-6 g daily in divided doses (this approach has more recently been reported to be not very effective).
- Budesonide (9 mg/day) is effective for diseases confined to the ileum and/or right colon.
- Proton pump inhibitors might help with symptomatic improvement in patients with upper gastrointestinal Crohn's disease.
Moderate to Severe Disease
- Prednisone 40-60 mg/day until resolution of symptoms.
- Appropriate antibiotic therapy for infection or abscess.
- Azathioprine and 6-MP are effective for maintaining steroid-induced remission.
- Methotrexate 25 mg/wk is effective for steroid-dependent and steroid-refractory Crohn's disease.
- Infliximab, adalimumab, and certolizumab pegol are effective in the treatment of moderate to severely active disease in patients who have not responded to adequate therapy with a steroid or immunosuppressive agent.
- Natalizumab is effective in the treatment of patients with moderate to severely active CD who have had an inadequate response or are unable to tolerate conventional Crohn's disease therapy and anti-TNF antibody therapy.
Perianal or Fistulizing Disease
- Surgical drainage for abscess
- Otherwise, treated medically with antibiotics (metronidazole), immunosuppressives, or infliximab.
What vaccinations are recommended for Crohn's disease?
Vaccination recommendations for individuals with Crohn's disease include the following:
- Adults with inflammatory bowel disease generally should follow the same vaccination schedules as the general population.
- They should receive a single dose of Tdap, then a Td booster every 10 years.
- Women between the ages of 9 and 26 should receive 3 doses of the HPV vaccine (and consideration should be given to older patients who are HPV negative on Pap smear). Men in the same age range should also consider being vaccinated given the increased risk of HPV with immunosuppression.
- Influenza (flu) vaccine should be given annually to all patients (though the live intranasal vaccine is contraindicated in patients on immunosuppressive therapy).
- One dose of pneumococcal vaccine should be given between age 19-26 and then revaccination after 5 years.
- If not previously vaccinated, all adults should receive 2 doses of hepatitis A vaccine and 3 doses of hepatitis B.
- The meningococcal vaccine is only recommended for patients with anatomic or functional asplenia, terminal complement deficiencies, or others at higher risk (college students, military recruits, etc.).
- Mumps/measles/rubella, varicella, and zoster vaccines are contraindicated for patients on biologic therapy, as they are all live vaccines.
- COVID-19: People with IBD or Crohn's are not at increased risk for severe illness from COVID-19. Most people with IBD respond well to the COVID-19 vaccine and are not at an increased risk of infection or hospitalization, according to the Crohn's and Colitis Foundation.
Other factors that may affect Crohn's disease
- A study found that smoking is a risk factor for Crohn's disease, and secondhand smoke also can contribute to a worse prognosis. Quitting smoking should be advised for patients with Crohn's disease.
- Osteoporosis with markedly reduced bone mineral densities has also increasingly been recognized as a significant health problem in patients with inflammatory bowel disease. Screening with a bone density study is recommended in postmenopausal women, men over age 50, patients with prolonged corticosteroid use (more than 3 consecutive months or recurrent courses), patients with a personal history of traumatic fractures with minimal trauma, and patients with hypogonadism.
- Most patients with inflammatory bowel disease should be taking calcium and vitamin D supplements.
What is the Crohn's disease diet?
Dietary changes and supplementation that may help control Crohn's disease include:
- Since fiber is poorly digestible, it can worsen the symptoms of intestinal obstruction. A low-fiber diet for Crohn's disease may be recommended, especially in those patients with small intestinal disease.
- A liquid diet may be of benefit when symptoms are more severe.
- Intravenous nutrition or TPN (total parenteral nutrition) may be utilized when it is felt that the intestine needs to "rest."
- Supplementation of calcium, folate, and vitamin B12 is helpful when malabsorption of these nutrients is apparent.
- The use of anti-diarrheal agents (diphenoxylate and atropine [Lomotil], loperamide [Imodium]) and antispasmodics also can help relieve symptoms of cramps and diarrhea.
Can Crohn's disease be cured?
There is no cure for Crohn's disease, only treatments for pain and other symptoms.
Crohn's disease is a chronic inflammatory disease involving predominantly the small intestine and colon. The symptoms and the activity of the disease can come and go. Even though many effective medications are available to control the activity of the disease, there is as yet no cure for Crohn's disease.
Surgery can significantly improve the quality of life in selected individuals, but recurrence of the disease after surgery is common.
Crohn's disease can have complications, both within and outside of the intestine. Newer treatments are actively being evaluated.
A better understanding of the role of genetics and environmental factors in the cause of Crohn's disease may lead to improved treatments and prevention of the disease.
What are the complications of Crohn's disease? Is it fatal?
Complications of Crohn's disease may be related or unrelated to the inflammation within the intestine, and may include the following:
- Intestinal complications of Crohn's disease include:
- Obstruction and perforation of the small intestine
- Abscesses (collections of pus)
- Fistulae
- Intestinal bleeding
- Massive distention or dilatation of the colon (megacolon), and rupture (perforation) of the intestine are potentially fatal complications. Both generally require surgery, but, fortunately, these two complications are rare. Recent data suggest that there is an increased risk of cancer of the small intestine and colon in patients with long-standing Crohn's disease.
- Extra-intestinal complications involve the skin, joints, spine, eyes, liver, and bile ducts.
- Skin involvement includes painful red raised spots on the legs (erythema nodosum) and an ulcerating skin condition generally found around the ankles called pyoderma gangrenosum.
- Painful eye conditions (uveitis, episcleritis) can cause visual difficulties.
- Arthritis can cause pain, swelling, and stiffness of the joints of the extremities.
- Inflammation of the lower back (sacroiliac joint arthritis) and of the spine (ankylosing spondylitis) can cause pain and stiffness in the spine.
- Inflammation of the liver (hepatitis) or bile ducts (primary sclerosing cholangitis) also can occur. Sclerosing cholangitis causes narrowing and obstruction of the bile ducts draining the liver and can lead to yellow skin (jaundice), recurrent bacterial infections, and liver cirrhosis with liver failure. Sclerosing cholangitis with liver failure is one of the reasons for performing liver transplantation. It also is frequently complicated by the development of cancer of the bile ducts. Patients with Crohn's disease might also suffer from an increased tendency to form blood clots (hypercoagulability).
Top Crohn's Disease Related Articles

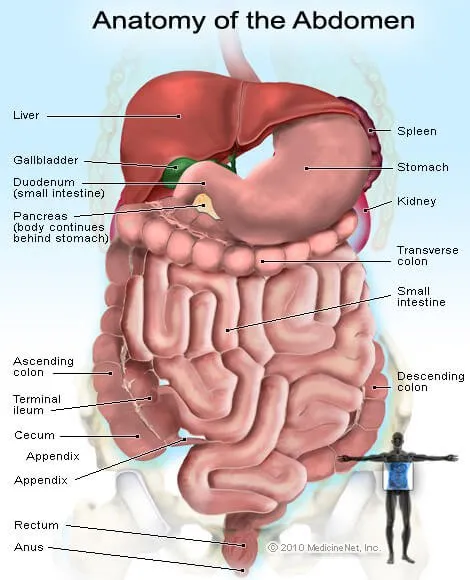
Abdomen Picture
The abdomen (commonly called the belly) is the body space between the thorax (chest) and pelvis. See a picture of the Abdomen and learn more about the health topic.
What's Causing Your Abdominal Pain?
In general, abdominal pain, which may be in the lower left or right of your abdomen, is a symptom of many possible conditions including appendicitis, ulcers, irritable bowel syndrome, indigestion, and others. It may accompany constipation, diarrhea, vomiting, and other symptoms. Find out the potential causes of pain in the abdomen and learn when you should see a doctor.
Biological Therapy
Biological or biologic therapy is a type of treatment used to stimulate or restore the ability of the body's immune system. Other names for this type of therapy include biotherapy or immunotherapy. It is used to treat cancer and other conditions, as it helps the body fight infection and disease.
C-Reactive Protein (CRP) Test
What are the ranges and levels of C-Reactive protein (CRP) in the blood? The CRP blood test is a marker of inflammation in the body, and it is produced by the liver. Find out about high, low, and normal ranges, levels, and results.
Colonoscopy
A colonoscopy is a procedure whereby a docotor inserts a viewing tube (colonoscope) into the rectum for the purpose of inspecting the colon. Colonoscopy is the best method currently available to diagnose, detect, and treat abnormalities within the colon.
Crohn's Disease Quiz
What causes Crohn's disease? What are the symptoms of Crohn's disease? How is Crohn's treated? Take this quiz to get the facts about Crohn's.
Crohn's Disease: Symptoms, Causes, Diet
What is Crohn's disease? Get more information on this digestive disorder and how Crohn's can affect your diet. Learn more about tests to diagnose Crohn's disease, as well as treatments for Crohn's.
Diarrhea
Diarrhea is a change in the frequency and looseness of bowel movements. Symptoms associated with diarrhea are cramping, abdominal pain, and the sensation of rectal urgency. Causes of diarrhea include viral, bacterial, or parasite infection, gastroenteritis, food poisoning, and drugs. Absorbents and anti-motility medications are used to treat diarrhea.
Gastritis
Gastritis (acute and chronic) is an inflammation of the lining of the stomach Some people have no gastritis symptoms, but when they do occur they may include bloating, belching, loss of appetite, nausea, and vomiting. H. pylori infection and nonsteroidal anti-inflammatory drugs (NSAIDs) are the two main causes of gastritis. Alcohol, caffeine, and high-fat foods also can cause gastritis. Fried, fatty, and spicy foods and alcohol aggravate gastritis symptoms. Other stomach lining irritants that aggravate symptoms include cigarette smoking, acidic juices, caffeine, tomato products, peppers, and chili powder. Foods that soothe gastritis symptoms, and that help reduce and stop H. pylori infection growth in the stomach includes apples, onions, garlic, teas, green leafy vegetables, coconut water, and wheat bran. Gastritis is diagnosed with endoscopy, blood tests, or stool tests. Some people get relief from gastritis symptoms with prescription and non-prescription antacids, histamine blockers like famotidine (Pepcid AC) or ranitidine (Zantac 75), or proton pump inhibitors (PPIs) like omeprazole (Prilosec) and esomeprazole (Nexium). These drugs will not cure gastritis. Complications of gastritis include gastric cancers, MALT lymphoma, renal problems, and death.
IBD Slideshow
What is inflammatory bowel disease? IBD can include Crohn's disease and ulcerative colitis. Learn more about testing, treatments, and the home care needed to manage inflammatory bowel disease.
Liver Blood Tests
An initial step in detecting liver damage is a simple blood test to determine the presence of certain liver enzymes in the blood. Under normal circumstances, these enzymes reside within the cells of the liver. But when the liver is injured, these enzymes are spilled into the bloodstream and can lead to diseases like fatty liver, type 2 diabetes, obesity, and hepatitis. Several medications also can increase liver enzyme test results.
Night Sweats
Night sweats are severe hot flashes that occur at night and result in a drenching sweat. The causes of night sweats in most people are not serious, like menopause in women, sleep apnea, medications, alcohol withdrawal, and thyroid problems. However, more serious diseases like cancer and HIV also can cause night sweats. Your doctor will treat your night sweats depending upon the cause. You may experience other signs and symptoms that are associated with night sweats, which depend upon the cause, but may include, shaking, and chills with a fever caused by an infection like the flu or pneumonia; unexplained weight loss due to lymphoma; women in perimenopause or menopause may also have vaginal dryness, mood swings, and hot flashes during the day; and low blood sugar in people with diabetes. Other causes of night sweats include medications like NSAIDs (aspirin, acetaminophen, ibuprofen (Motrin, Advil), and naproxen (Aleve, Naprosyn), antidepressants, sildenafil (Viagra), and abuse of prescription or illegal drugs and drug withdrawal; hormone disorders like pheochromocytoma and carcinoid syndrome; idiopathic hyperhidrosis; infections like endocarditis, AIDs, and abscesses; alcoholism and alcohol withdrawal; drug abuse, addiction, and withdrawal; and stroke. A doctor or other health care professional can treat your night sweats after the cause has been diagnosed.
Steroid Drug Withdrawal
Corticosteroid drugs such as prednisone and prednisolone are commonly used to treat asthma, allergic reactions, RA, and IBD. Steroids such as these do have serious drawbacks such as steroid withdrawal symptoms such as: fatigue, weakness, decreased appetite, weight loss, nausea, vomiting, abdominal pain, and diarrhea. Speak with your health care provider prior to tapering off steroid medications.
Stool Color Changes
Stool color changes can very from green, red, maroon, yellow, white, or black. Causes of changes of stool color can range from foods a person eats, medication, diseases or conditions, pregnancy, cancer, or tumors. Stool can also have texture changes such as greasy or floating stools. Stool that has a uncharacteristically foul odor may be caused by infections such as giardiasis or medical conditions.
Tuberculosis PPD Skin Test
The tuberculosis skin test (also known as PPD, tuberculin, or Mantoux) determines whether a person has developed an immune response to the bacterium that causes tuberculosis (TB). Learn how doctors administer the TB test, obtain a reading, and interpret the results.
Tummy Trouble Quiz
Tummy Troubles? Get a better idea of what's causing the nausea, vomiting, bloating, gas, constipation, diarrhea, pain, and other gastrointestinal discomforts and problems. Take the Tummy Troubles Quiz!
Ulcerative Colitis
Ulcerative Colitis is a form of inflammatory bowel disease and is slightly different than Crohn's disease. Learn the causes, symptoms, diet, and treatment options associated with ulcerative colitis.